But Many Educators Still Don’t Understand Social-Emotional Screeners, and the Limitations of ACEs-Only Assessments
[CLICK HERE to read this Blog on the Project ACHIEVE Webpage]
Dear Colleagues,
Introduction
In my July 27, 2024 Blog a few months ago, I discussed the results of a recent School Pulse Panel survey organized by the National Center for Education Statistics (NCES). Completed between May 14 and May 28, 2024, the survey involved 1,714 public school K-12 leaders from every state in the country and Washington, D.C. focusing on their perspectives of the most compelling social, emotional, behavioral, and mental health concerns in their schools.
The article reported that the survey’s respondents identified a significant and wide variety of challenges in these areas. . . results echoed this past year in other research and national reports.
For example:
· 83% reported that the pandemic and its lingering effects continue to negatively influence the social-emotional development of students;
· 76% of the public school leaders said they need “more support for student and/or staff mental health”;
· 75% reported that students’ lack of focus or inattention had either a “moderate” or “severe” negative impact on learning during the 2023-24 school year;
· 71% need “more training on supporting students’ socioemotional development;”
· 45% reported having confiscated a weapon from students during the year;
· 36% reported that student acts of disrespect toward teachers or staff members, other than verbal abuse, occurred at least once a week;
· 30% reported instances of cyberbullying that happened at and outside of school at least once a week; and
· 20% reported that threats of physical attacks or fights between students occurred at least once a week.
From a screening perspective, some schools use specific assessments or tools to identify students with possible social, emotional, or behavioral challenges that need follow-up.
It is critical to note—right from the beginning—that Educators:
· Read the technical manuals for social-emotional screening tools they are considering to determine if they are well-normed, reliable and valid, and applicable to the students in their specific schools;
· Recognize that screening tools are not diagnostic tools that are sensitive enough to differentially determine the specific social-emotional concerns or interventions needed by a student;
· Reflect that screening tools result in False-Positive and False-Negative results—where students are incorrectly identified as having a “problem” (that does not exist), or as not having a “problem” (where one actually exists), respectively; and
·
Remember that screening tools must be followed up by
diagnostic assessments that both validate the screening tool’s results, and
determine the specific clinical concerns presented by a student.
_ _ _ _ _
The ACEs
One screening tool area that has received a fair amount of attention over the recent years measures students’ Adverse Childhood Experiences (ACEs).
There are serious concerns with these scales in that some believe that: (a) the ACEs areas reliably, validly, and diagnostically assess “traumatic” events in students’ lives; (b) a high number of ACEs events or scores predicts individuals who will exhibit current or eventual social, emotional, behavioral, and mental health challenges; and that (for the very uninformed) (c) this relationship is causal, as opposed to correlational (and what that means).
Through this Blog, we want to make sure that every educator understands what an ACEs scale is really measuring, and we report on a recent study that begins the process of helping us understand what an ACEs screening survey score may actually correlate with in our classrooms and schools.
As we try to “cut through the talk,”
we hope to solidify educators’ understanding that an ACEs screening has more
limitations than strengths relative to their applicability to classrooms and schools.
_ _ _ _ _ _ _ _ _ _
What the ACEs Research Is and Isn’t
The original ACEs Study was conducted by the Kaiser Permanente Health Maintenance Organization (HMO) in Southern California from 1995 to 1997 with two waves of data collection. As they were receiving physical exams, over 17,000 HMO members completed confidential surveys regarding their childhood experiences and their current health status and behaviors. Significantly, beyond the fact that the sample was from a limited geographic area, the participants were primarily white and from the middle class.
Below are the actual ACEs Study Questions. Each “Yes” response received one point toward the “final score.” As educators, please read these items relative to today’s students. Think about how many of your students have experienced four or more of these events so far in their lives (more on that below).
While
you were growing up, during your first 18 years of life:
1.
Emotional Abuse. Did a parent or other adult in the household often or
very often… Swear at you, insult you, put you down, or humiliate you?
or
Act in a way that made you afraid that you might be physically hurt?
2.
Physical Abuse. Did a parent or other adult in the household often or
very often… Push, grab, slap, or throw something at you?
or
Ever hit you so hard that you had marks or were injured?
3.
Sexual Abuse. Did an adult or person at least 5 years older than you
ever…
Touch
or fondle you or have you touch their body in a sexual way?
or
Attempt or actually have oral, anal, or vaginal intercourse with you?
4.
Emotional Neglect. Did you often or very often feel that … No one in
your family loved you or thought you were important or special?
or
Your family didn’t look out for each other, feel close to each other, or
support each other?
5.
Physical Neglect. Did you often or very often feel that … You didn’t
have enough to eat, had to wear dirty clothes, and had no one to protect you?
or
Your parents were too drunk or high to take care of you or take you to the
doctor if you needed it?
6.
Parental Separation or Divorce. Were your parents ever separated or
divorced?
7.
Mother Treated Violently. Was your mother or stepmother: Often or very
often pushed, grabbed, slapped, or had something thrown at her?
or
Sometimes, often, or very often kicked, bitten, hit with a fist, or hit with
something hard?
or
Ever repeatedly hit at least a few minutes or threatened with a gun or knife?
8.
Household Substance Abuse. Did you live with anyone who was a problem
drinker or alcoholic or who used street drugs?
9.
Household Mental Illness. Was a household member depressed or mentally
ill, or did a household member attempt suicide?
10.
Incarcerated Household Member. Did a household member go to prison?
_ _ _ _ _
Initially, it is paramount to remind educators that “Trauma” is clinically defined—from a psychological/psychiatric perspective—and it is diagnostically differentiated from related mental health challenges like stress, anxiety, and fear.
We have discussed this in a previous Blog, showing that the clinical definition and criteria for a diagnosis of “trauma” is far more narrow than the way it is represented in the popular press.
Indeed, given the criteria, there are far fewer children, adolescents, and adults who are clinically traumatized than reported in the popular press, and when contrasted with individuals clinically affected by stress, anxiety, or fear.
To read more about this, go to:
August 8, 2020
Why Stress-Informed Schools Must Precede Trauma-Informed Schools: When We Address Student Stress First, We Begin to Impact Trauma. . . If It Exists
_ _ _ _ _
Continuing the ACEs discussion begun above:
The most critical concerns with the ACEs Questions are:
· They do not discriminate between “finite” events (e.g., having a household member incarcerated) and events that can occur over time or in a repeated way;
· Thus, they do not quantify many of the events (e.g., how long was the separation, how many times was your mother physically threatened);
· They do not identify the age (or age range) when the child or adolescent experienced each event;
· They do not ask for a rating of the intensity of each event (e.g., along a Mild-Moderate-Severe continuum);
· They do not get a rating of the emotional impact of each event at the time that it occurred (e.g., along a None-Low-Mild-Moderate-Significant-Life Changing continuum); and
· They do not get a rating of the current (assuming an event occurred in the past) and/or continuing emotional impact of each event.
This leads to a critical conclusion:
Given
the absence of this critical contextual information, educators (and others) do
not really know the cumulative depth, breadth, intensity, or impact of an
individual’s projected traumatic history from an ACEs screening.
Indeed,
the screening may simply tell us how many challenging events an individual may
have experienced. It does not tell us if one or more of the events were
traumatic for an individual, or if they continue to be traumatic.
_ _ _ _ _
Briefly, the results of the original ACEs study indicated that:
·
About two-thirds of participants
reported at least one adverse childhood experience;
· The number of ACEs points were strongly
associated with high-risk health behaviors during adulthood such as smoking,
alcohol and drug abuse, promiscuity, and severe obesity;
· The number of ACEs points also
correlated with depression, heart disease,
cancer,
chronic lung disease, and a shortened
lifespan.
· Compared to an ACEs score of zero,
having four adverse childhood experiences (i.e., Four or more ACEs points) was
associated with a seven-fold (700%) increase in alcoholism,
a doubling of risk of being diagnosed with cancer, and a four-fold increase in emphysema;
and
· An ACEs score above six was associated with a 30-fold (3,000%) increase in attempted suicide.
More than 50 ACEs-related studies have followed the original. These studies have (a) used more diverse and different participant samples—including children and adolescents as respondents; (b) looked at different physical, behavioral, mental health, and life outcomes; (c) adapted the original ACE survey and methodology; and (d) replicated many of the correlational (not causal) results from the original study.
In addition, the concerns highlighted by these studies resulted—starting in 2011 in Florida—in communities beginning trauma-awareness programs; and—about 10 years ago in Massachusetts, Washington, and California—in schools beginning similar trauma-related initiatives.
Relative to prevention, a 2016 Center for Disease Control and Prevention Monograph made the following recommendations:

_ _ _ _ _
Critically, as noted, the ACEs surveys or scales reviewed are screening tools that are not very sensitive and may, in fact, be biased in their attempts to correlate a number of challenging events in students’ lives with their current social, emotional, behavioral, or mental health status.
In point of fact, an ACEs scale:
· Is not a reliable or valid diagnostic instrument;
· It cannot draw causal connections between any number of challenging life events and a student’s current social, emotional, or behavioral status; and
· If used as the only social-emotional screener by a school, it has a high potential of both over-identifying some students, while under-identifying others.
If a district or school wants to
use a social, emotional, behavioral screening tool (which is not necessarily
recommended in all cases), there are a number of far more effective,
psychometrically-sound tools available. . . that provide information and
context well beyond the current ACEs screeners.
_ _ _ _ _ _ _ _ _ _
Kindergarten Readiness Not Impacted by a High Number of ACEs
Earlier this month (September 11, 2024), an article was published in K12 Dive reviewing a study published in the Journal of Child and Family Studies involving 115 preschoolers attending a comprehensive school readiness summer program in Miami in 2017, 2018, and 2019. The children were transitioning between preschool and kindergarten, and they were enrolled because they were exhibiting disruptive behavior problems at home and in school.
After completing an ACEs survey with the children’s parents or caregivers, the study reported that nearly all of the children had experienced poverty, about 94% had experienced at least one ACE, and 49% had experienced four or more ACEs. Only 6% of the children in the study had experienced no ACEs.
The K12 Dive article summarized the study’s results and implications as follows:
· The study found a correlation between
the number of adverse childhood experiences faced by rising kindergartners and
the severity of their disruptive behaviors, anxiety, and depression.
· But, the correlation between the ACEs and the students’ performance did not hold for the students’ academic and social readiness, with those skills being comparable with peers experiencing fewer harmful events.
During an interview with the study’s lead author, she noted that the
ACEs’ correlation with students’ internalizing and disruptive behavior was
expected, but she was surprised that there was no association between a
student’s ACEs score and his or her academic functioning, for example, in early
math and reading skills.
_ _ _ _ _ _ _ _ _ _
ACEs Implications and Practical Next Steps
This study provides educators both good news and bad news.
The good news is that research is starting (continuing) to investigate the functional relationship between the number of ACEs experienced by a student and a variety of academic and social, emotional, behavioral, and mental health outcomes.
The bad news (for some believing that ACEs screenings portend important school outcomes) is that—while this study focused only on a relatively small number of very young students in one geographic area—it, as above, (a) confirmed a logical and expected correlation between the ACEs and participating students’ emotional and behavioral status, but (b) rejected what many educators assumed would be a similar ACEs correlation with their academic status.
As noted earlier, we cannot conclude from even the one confirmed correlation above that a high ACEs score means that a student is “traumatized,” or that any of the ACEs events were the reasons behind a student’s current social, emotional, behavioral, or mental health status.
Indeed, to really understand the results of this study, every student considered “at-risk” by the ACEs screener would need to be diagnostically assessed to determine exactly what appropriate and challenging behaviors they were demonstrating and when during the school day, as well as why the challenging behaviors were occurring (i.e., the root causes) and how they were being triggered.
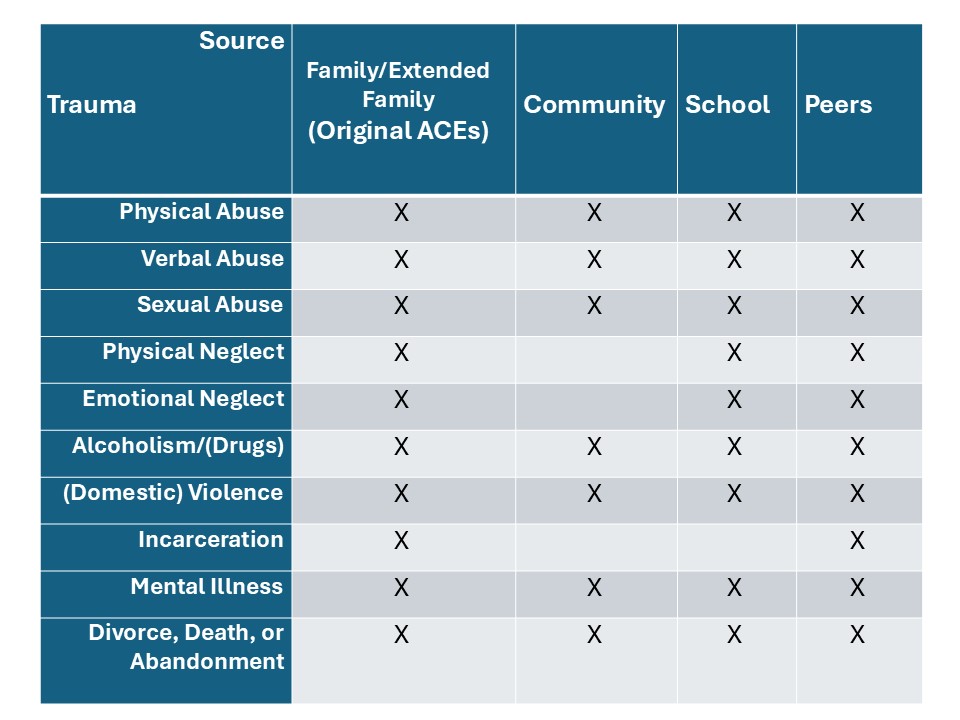
Critically, students’ social, emotional, and behavioral challenges are triggered in many different ways— often well beyond any of the events described in an ACEs screener. Indeed, if you re-read the ACEs screening questions above, you will note that the vast majority of the items focus on home and family-related events.
Below is a table with the original ten ACEs areas, and X’s in boxes indicating that many of the ACEs events could occur in Community or School settings, as well as with or due to Peers.
The point here is that: The ACEs events or issues are not limited to our students’ familial experiences. Moreover, social, emotional, behavioral, and mental health assessments need to include multiple student settings, sources, and events.
Said a different way:
Trauma, stress, anxiety, and other social-emotional issues are not setting-specific. They are event-dependent. Events obviously can be experienced outside of the family or home, and they can be just as emotionally debilitating as those measured by an ACEs screening.
_ _ _ _ _
But even beyond the ACEs events above, there are many other life experiences that trigger students’ social, emotional, and interpersonal challenges.
These may include:
·
Academic Frustration
·
Test/Homework/Work Completion Anxiety
·
Peer (including Girlfriend/Boyfriend) Conflicts/Rejection
·
Teasing and Bullying—Direct, Indirect, Social, and Social
Media
·
Gender Status or Discrimination
·
Racial or Multi-Cultural Status or Discrimination
·
Sexual Identification or Orientation Discrimination
·
Socio-economic Status or Discrimination
·
Circumstances Related to Poverty/Parental Income
·
Family Moves/Housing Mobility/Homelessness
·
Competition/Losing
· Physical or Other Limitations or Disabilities
On a situational level, these triggers can product emotional reactions that are just as quick and intense as those that are family- or trauma-related, and these events need to be consciously factored into a social, emotional, or behavioral screening.
The Take-Aways here include the following:
· There are multiple circumstances or events that trigger students’ emotionality in school. Many of them are not specifically (or by definition) traumatic events and, thus, schools that are too focused on trauma may easily miss them.
· Schools need to assess and identify the emotional triggers that are most prevalent across their students, and they should target these emotional triggers with their preventative services, supports, and interventions.
At the Tier 1 level, these triggers need to be integrated into the schools’ social skills curricula at the prevention and early response levels.
At the Tier 2 and 3 levels, these triggers need to frame the strategic or intensive interventions or therapies that related services personnel prepare to deliver.
· Finally, schools and districts need to be prepared to deliver the full multi-tiered continuum of services, supports, strategies, and interventions for students with social, emotional, behavioral, and mental health challenges. This includes the necessary training, resources, and personnel both in general, and as needed on a year-to-year basis.
Some of the Tier 2 or 3 clinical interventions that may be needed at the deeper levels of the multi-tiered continuum include:
·
Progressive Muscle Relaxation Therapy and Stress Management
· Emotional Self-Management (Self-awareness, Self-instruction, Self-monitoring, Self-evaluation, and Self-reinforcement) Training
·
Emotional/Anger Control and Management Therapy
·
Self-Talk and Attribution (Re)Training
·
Thought Stopping approaches
·
Systematic Desensitization
·
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT)
·
Cognitive-Behavioral Intervention for Trauma in Schools
(CBITS)
· Structured Psychotherapy for Adolescents Responding to Chronic Stress (SPARCS)
· Trauma Systems Therapy (TST)
Ultimately, districts and schools need to ask themselves:
Do
your related service professionals have the skills to clinically deliver (as
needed, and based on student-centered diagnostic assessments) some or all of
the strategies or therapies above. . . and/or, are they available from the
mental health professionals who are practicing in your community?
_ _ _ _ _ _ _ _ _ _
Summary
We started this Blog journey by revisiting the many social, emotional, behavioral, and mental health concerns this past school year as documented by the National Center for Education Statistics. While many of these concerns have existed for years, the striking outcome is their elevation especially due to the pandemic.
To analyze these concerns on a local level, many districts use a social-emotional screening process with their entire student populations. Critically, the Blog discussed the limitations of these screening instruments, emphasizing that they make errors, and that all screening results must be validated through individual student diagnostic assessments.
The Blog then focused on screeners that assess for students’ Adverse Childhood Experiences (ACEs). We detailed the history, psychometric properties, and research with ACEs assessments, noting serious limitations with their validity and ability to causally explain students’ social-emotional difficulties. We concluded that ACEs screeners are not good assessments for root cause analyses or to ecologically measure traumatic life events.
We reviewed a recently published study analyzing preschool to first grade students that found the ACEs correlated with social-emotional but not academic performance. We identified the many reasons (beyond traumatic events) that explain students’ social-emotional challenges, and discussed some of the Tier 2 and 3 interventions available to help.
Our ultimate conclusion was that:
We cannot conclude that a high ACEs score
means that a student is “traumatized,” or that any of the ACEs events were the
reasons behind a student’s current social, emotional, behavioral, or mental
health status.
ACEs surveys are screening tools. Given
the absence of critical contextual information within the individual events
assessed through the ACEs’ items, educators (and others) do not really know the
cumulative depth, breadth, intensity, or impact of an individual’s projected traumatic
history from an ACEs screening.
Indeed, the screening may simply tell us how many challenging events an individual may have experienced. It does not tell us if one or more of the events were traumatic for an individual, or if they continue to be traumatic. This information can only come from an individual diagnostic assessment process that identifies past and present social, emotional, behavioral, and mental health status; the ecologically-based root causes of any significant challenges; and what specific evidence-based services, supports, and/or interventions link to specific root causes.
All of this is focused on helping schools to most effectively address the social, emotional, and behavioral needs of all students—with a focus on their corresponding self-management. When students have social, emotional, and behavioral self-management skills, and the peer, staff, and school support to facilitate them, issues related to—for example—stress, anxiety, fear, trauma and their emotional triggers become less evident. . . because they are handling, addressing, and coping with them.
Our
schools still have a ways to go. But teachers, support staff, and
administrators need the (right) training, professional development, and
support; and schools need to have the mental health and related service
colleagues. Otherwise, the gaps will
(continue to) undermine all of the best intentions, plans, and actions.
_ _ _ _ _
Now that everyone across the country has begun their school year, we hope that this Blog is helpful and relevant to your planning and implementation.
If you would like to discuss these issues (or others) with me as part of a free virtual consultation, please drop me an e-mail (howieknoff1@projectachieve.info) so we can set up a Zoom call to look at your needs and gaps . . . and how to close these gaps and attain the outcomes that you want for students and staff.
Together, I know that we can make this the school year that you want and that every student deserves.
Best,
Howie
[CLICK HERE to read this Blog
on the Project ACHIEVE Webpage]
No comments:
Post a Comment